Restless Sleep Disorder: My Take
An expert consensus on a newly recognized sleep disorder, restless sleep disorder (RSD), may provide a much-needed link between behavioral issues in children and sleep. The evidence is substantial for ages 6-18, though younger children can be included. Restless sleep may manifest as (i) poor school performance, (ii) daytime sleepiness, (iii) behavioral concerns, (iv) fatigue, (v) irritability, or (vi) hyperactivity. Other sleep disorders, namely, sleep apnea, restless legs syndrome, and insufficient sleep, also have similar symptoms. Since RSD was previously not a recognized entity, many children did not meet diagnostic criteria for the other sleep disorders mentioned leaving many untreated or mistreated.
The proposed diagnostic criteria for RSD:
- Complaint of ‘restless sleep’ by the parent, caregiver, or patient;
- Large body movements involving either the whole body, all four limbs, arm, legs, or head (see Image 1);
- Occurs during sleep;
- At least three times a week;
- For three or more months;
- Video sleep study documenting more than five movements per hour;
- Impaired functioning, i.e., behavioral, educational, academic, social, occupational, or other important areas;
- Not adequately explained by another condition.
Attention deficit hyperactivity disorder (ADHD) and autism are conditions that seem to co-exist alongside RSD. The recognition of RSD may improve outcomes for patients with ADHD and autism by reducing the need and the dose of long-term medications. Some clinicians may even misdiagnose children with ADHD instead of RSD. We frequently come across a similar bidirectional effect between sleep and mental health issues in adults.

Patients who met the RSD criteria had lower overall sleep time, more awakenings in the middle of sleep, with no problems falling asleep. The shorter sleep time among RSD patients emphasizes the need for caregivers and parents to know the amount of sleep required for children. Further attention and inquiry into sleep habits by caregivers and clinicians should be essential in any pediatric visit, mainly when complaints are associated with behavioral, mood, or school performance. Restless sleep should be directly addressed by the parent or clinician as it unlikely the presenting complaint for the visit.
Treatment suggestions for RSD (following fasting iron panel bloodwork):
- Oral iron for 3- 6months, sometimes is poorly tolerated due to side effects and long treatment period, or
- [preferred] IV iron, one-time infusion, or
- Gabapentin
The proposed RSD is not another attempt to medicalize our health but to make sense of issues that have warranted medicating our children with stimulants such as Adderall. Without an exact cause of a patient or parent complaint – behavioral, mood, or school performance – most clinicians will opt to treat symptoms. Due to the health system’s pressure to see more patients for dwindling dollars, stimulants are a convenient tool to shorten visit times. Long term stimulants come with potential side effects, intended and unintended.
Providing clinicians a diagnostic framework and alternative treatment consideration will allow for more research on RSD and hopefully healthier, less heavily medicated children.
Image 1: Typical body movement types in children with RSD
Images taken during video-polysomnography demonstrating body movements in a child with RSD. Photos in the same row show the initial position during sleep, mid-movement position, and final position with the time spent in the movement (seconds). Images are taken with an infrared camera synchronized to the Polysomnogram at a sampling rate of 30 frames per second.
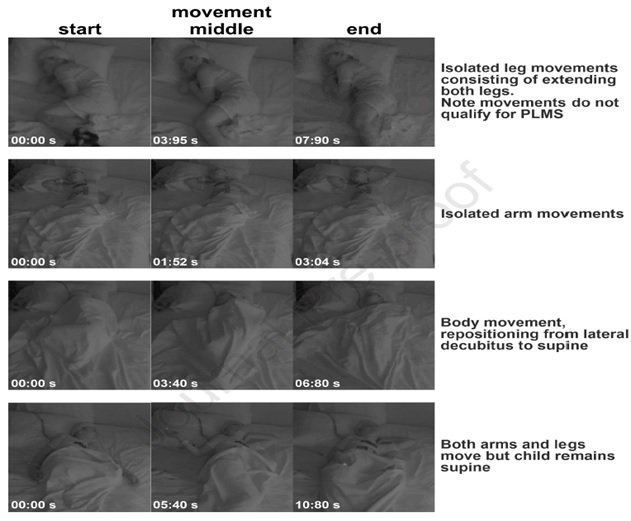
Image 1
Reference:
- DelRosso LM, Ferri R, Allen RP, Bruni O, Garcia-Borreguero D, Kotagal S, Owens JA, Peirano P, Simakajornboon N, Picchietti DL, On behalf of the International Restless Legs Syndrome Study Group (IRLSSG), Consensus diagnostic criteria for a newly defined pediatric sleep disorder: restless sleep disorder (RSD), Sleep Medicine, https://doi.org/10.1016/j.sleep.2020.08.011.
Written by: Avinesh S Bhar, MD MBA
Board-certified Sleep and Pulmonary Physician
Our sleep insomnia specialist, Dr. Avinesh Bhar, believes that high-quality care only comes from a trustful physician-patient relationship. With our telemedicine services Dr. Bhar can be your sleep insomnia doctor online.
